
Signal reproducibility
Test purpose
The aim of this multi-centre study was to test the ability of the system to detect small delivery errors in IMRT plans. This initial test in the study evaluated the short-term and long-term reproducibility of IQM measurements, because the research team considered strong reproducibility a basic requirement for any further analysis.
Test method
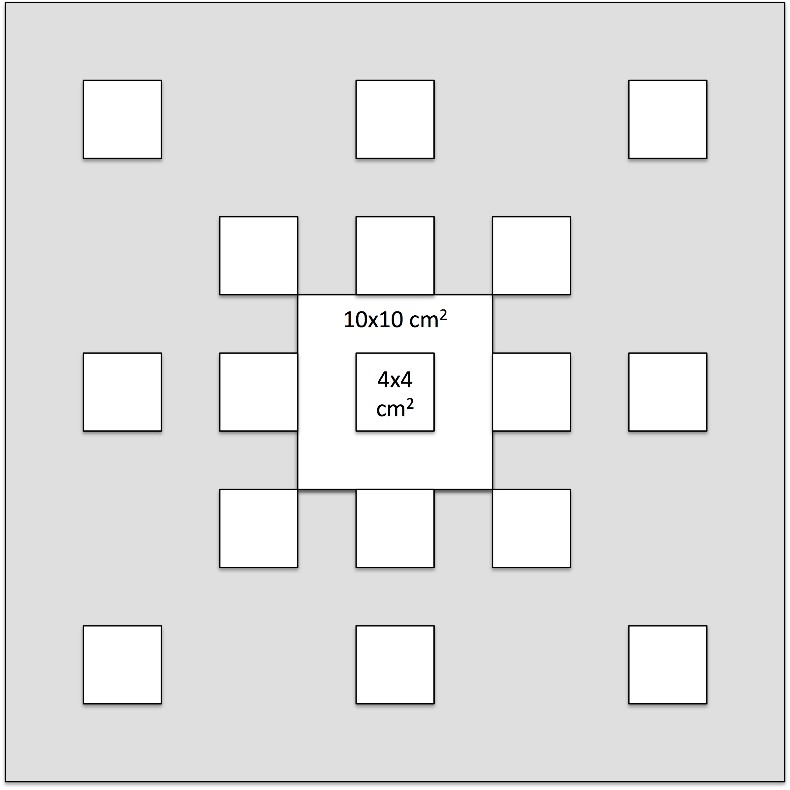
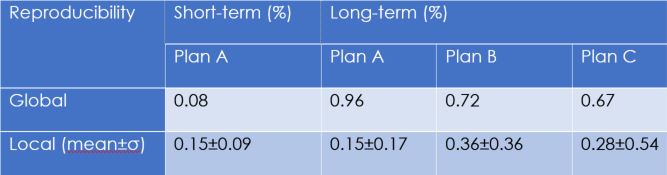
The short-term reproducibility was verified by delivering a test plan 15 consecutive times, over approximately 2 hours. The test field is a 6MV IMRT treatment field (treatment A) composed of 18 segments (17 4x4cm2 and one 10×10 cm2 field) (see figure 1). The output signal was analyzed segment by segment (local reproducibility) and for the entire field (global reproducibility).
The long-term detector reproducibility was evaluated by delivering three 6MV IMRT plans (A, B and C) at least 72 times each over a period of 30 days. Plans B and C are clinical plans for H&N and prostate treatment, respectively.

Conclusion
This test demonstrated the IQM system’s high short-term and long-term reproducibility. The larger multi-centre study found that the IQM system is capable of detecting small delivery errors in MU and leaf positions and shows a high sensitivity for clinical practice.

Correlation between IQM signal and DVH metrics
Test purpose
The aim of this multi-centre study was to test the ability of the system to detect small delivery errors in IMRT plans. Initial tests demonstrated the IQM system’s reproducibility and ability to detect the small errors introduced into IMRT plans. This test examined how the signal deviations detected by the IQM system for these small, induced errors correlate with variation in other commonly employed metrics for evaluating calculated and delivered dose distributions, such as the γ passing rate and DVH variations.
Test method
Seven types of errors were induced in 9 clinical step-and-shoot IMRT plans, by modifying the number of MUs and introducing small deviations in leaf positions. The original and modified plans were delivered and the detector signal variations were recorded. Calculated dose distributions were compared in terms of Gamma (γ) passing rates and Dose Volume Histogram (DVH) metrics (for several significant DVH parameters). The correlation between detector signal variations, γ passing rates and DVH parameters was investigated.
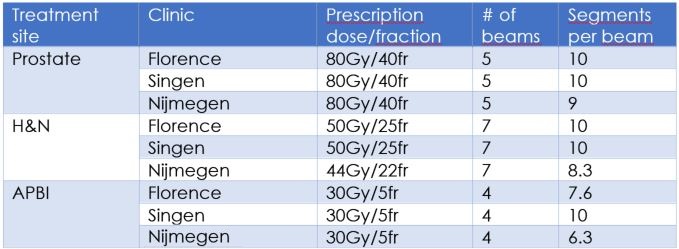
3 patients were selected for each of 3 anatomical sites, from which 24 plans for each anatomical site were generated: 3 “error free” (EF) plans (1 plan per patient) and 21 “error induced” (EI) plans (7 plans per patient). In total 72 plans were delivered and measured with the IQM system. For each EI plan delivery the IQM signal variations were recorded and the percentage variation with respect to the original EF plan delivery recorded signals was calculated.
For each EI plan, Gamma analysis (γ) was performed comparing the EI and EF dose distributions, and repeated with three levels of passing criteria: 3%/3mm, 2%/2mm and 1%/1mm. The correlation between γ pass rates and IQM signal variation was investigated.
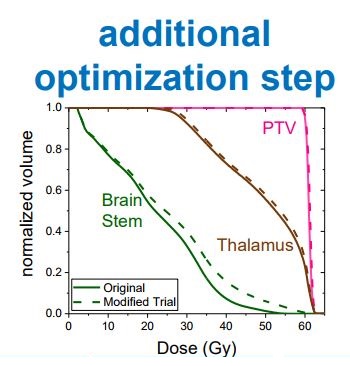
For each EI plan, DVH analysis was performed comparing the EI and EF dose distributions. The variations in several clinically relevant DVH parameters were evaluated for both PTVs and OARs. For PTVs, near maximum dose (D1%), D95% and V95% were recorded. The correlation between DVH parameter variation and IQM signal variation was investigated.
Test results
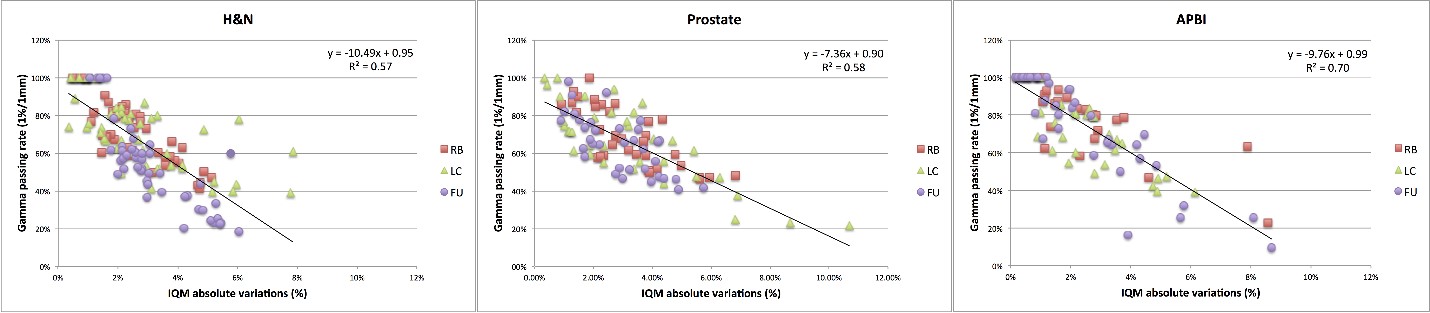
In the γ analysis, the induced errors were detected (passing rate < 100%) in a relatively low percentage of beams when the 3%/3mm and 2%/2mm criteria were applied. For the 3%/3mm criteria, the error detection percentages were: 58% for H&N, 36% for prostate and 29% for APBI. For the 2%/2mm criteria, the error detection percentages were 69% for H&N, 51% for prostate and 58% for APBI. Only for the 1%/1mm criteria were errors detected in the wide majority of beams (86% for H&N, 97% for prostate and 82% for APBI).
The following graph shows the γ passing rate (1%/1mm) as a function of the IQM percentage variation for each delivered beam of the H&N (a), prostate (b) and APBI (c) plans. As can be observed from the r2 values, the correlation between the γ passing rate (1%/1mm) and the IQM signal variation is moderate.
The next graph shows the correlation between PTV D95% and IQM signal variation for each treatment site, then the data for the 3 different sites plotted and fitted together.
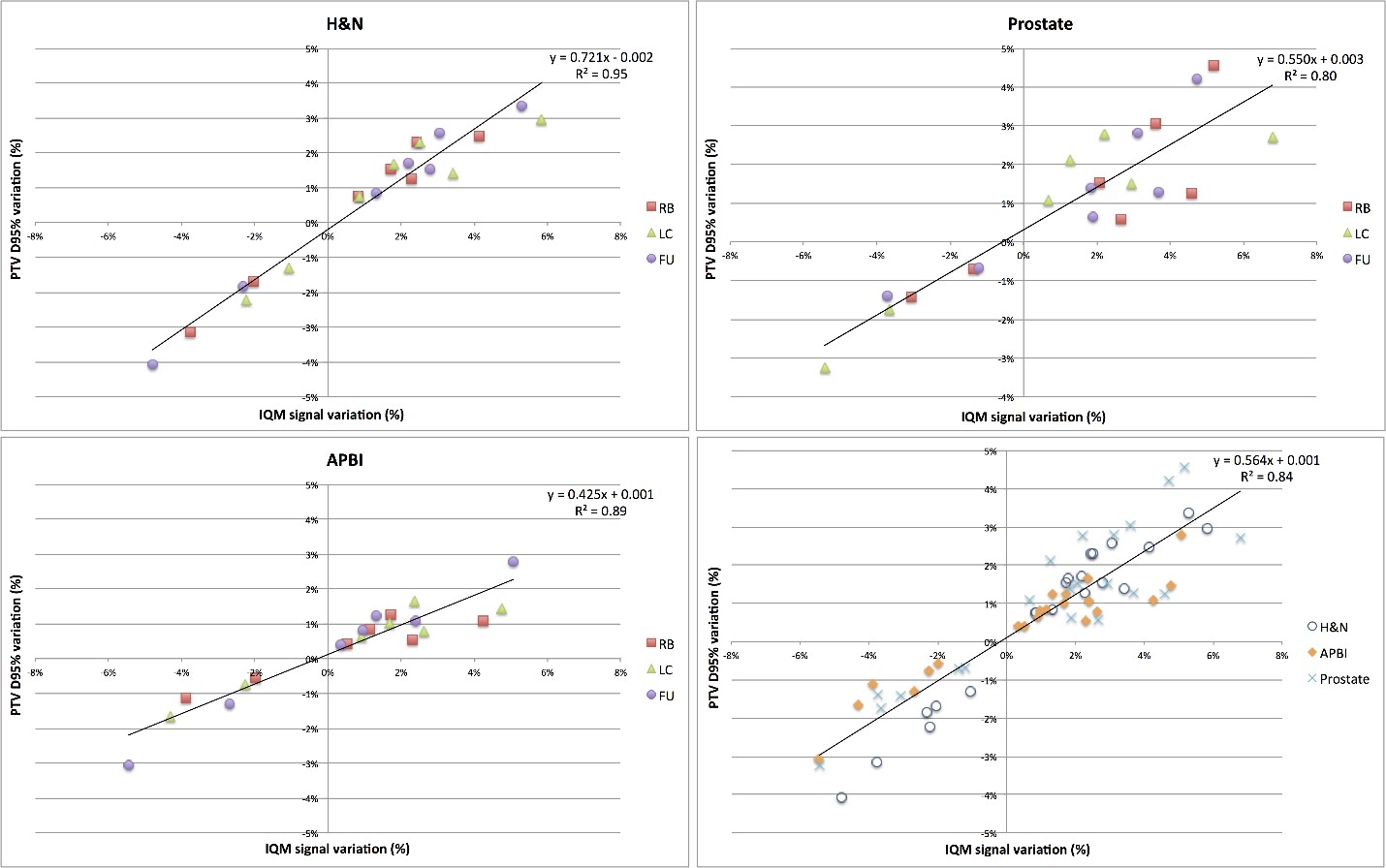
A good correlation exists between PTV D95% variation and IQM signal variation, independent of treatment site.
The following graph shows correlations between selected DVH OAR parameters and IQM signal variations.
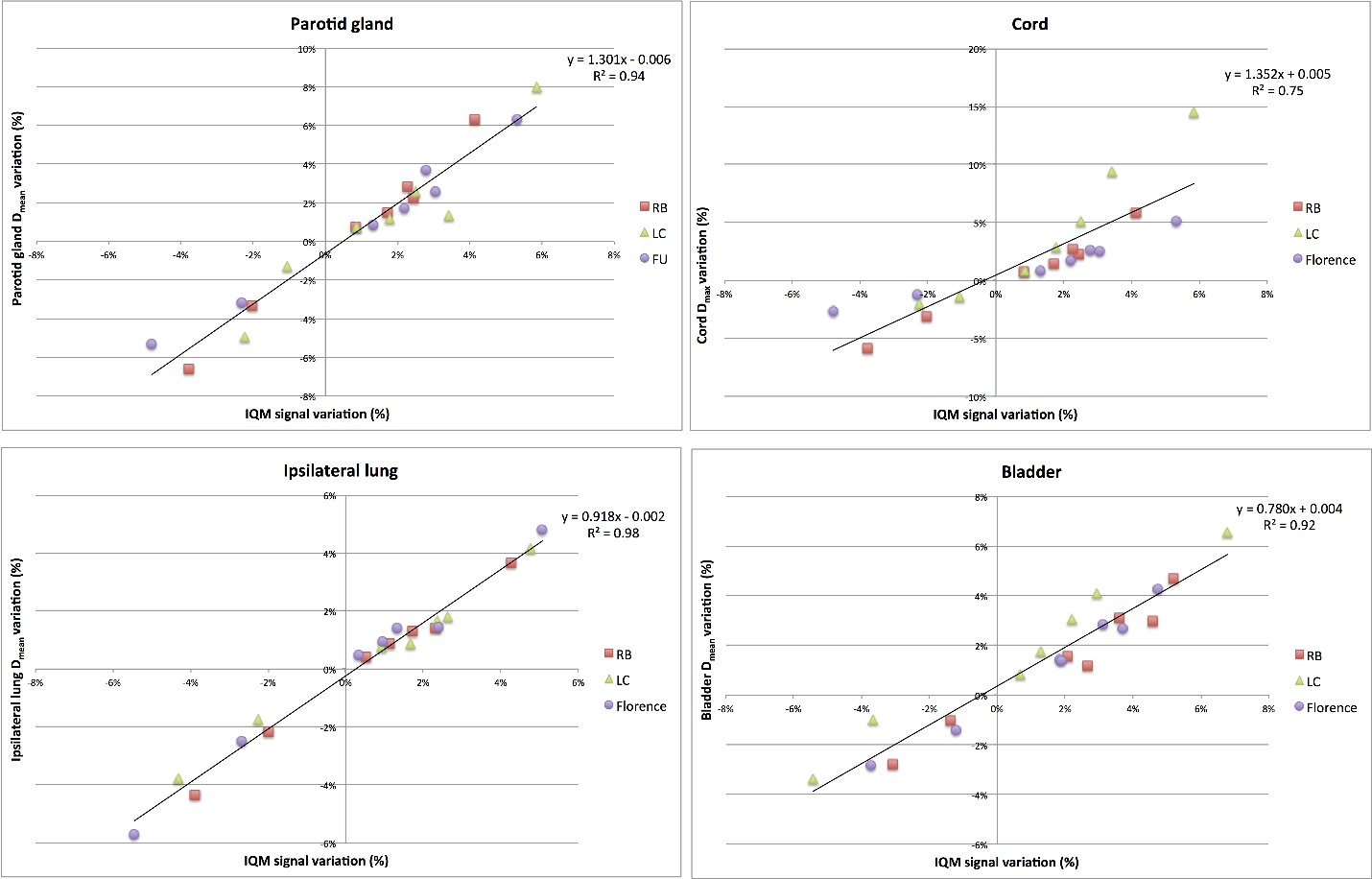
As can be observed by the correlation indices, PTV D95% and OAR’s Dmean are the DVH parameters expressing the best correlations with IQM signal variations. The data collected in the different centres were consistent, indicating a robust IQM performance.
The study found a good correlation between IQM signal variation, PTV D95% and several OAR parameter variations (especially Dmean) for the different treatment sites examined. Moreover, data collected in different centres, using different equipment and potentially different planning approaches, are consistent, demonstrating the robustness of the correlations found. This correlation makes it possible to identify DVH variation limits (associated with negligible or no clinical impact) for each individual patient and deriving corresponding IQM signal deviation tolerances.
Conclusion
This test demonstrated the IQM system’s clear and consistent correlation with DVH metrics. The larger multi-centre study found that the IQM system is capable of detecting small delivery errors in MU and leaf position and shows a high sensitivity for clinical practice.

Error detection sensitivity
Test purpose
This multi-centre study aimed to test the IQM system’s ability to detect small delivery errors in IMRT plans.
Test method
The researchers introduced 7 types of errors in 9 clinical step-and-shoot IMRT plans, by modifying the number of MUs and introducing small deviations in leaf positions. They delivered the original and modified plans and recorded the detector signal variations.
Each centre selected a patient case for each of 3 anatomical sites, and generated 8 plans for each patient: an “error free” (EF) plan and 7 “error induced” (EI) plans.
In total, the team delivered and measured 72 plans with the IQM system. They calculated dose distributions for each EF and EI plan, and determined each EI plan’s percentage variation with respect to the original EF dose distribution. They then compared the variation in the dose distributions to the corresponding variations in the recorded IQM signals for the EF and EI plans.
Test results
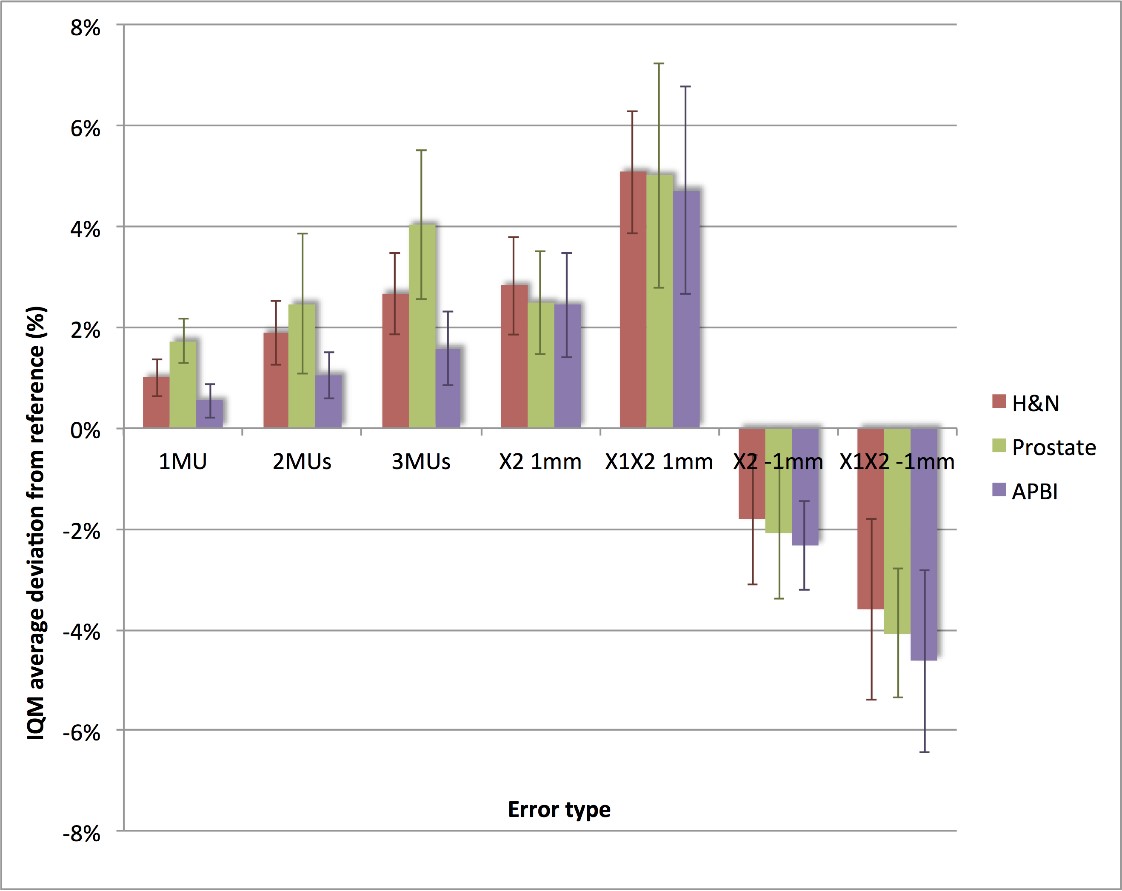
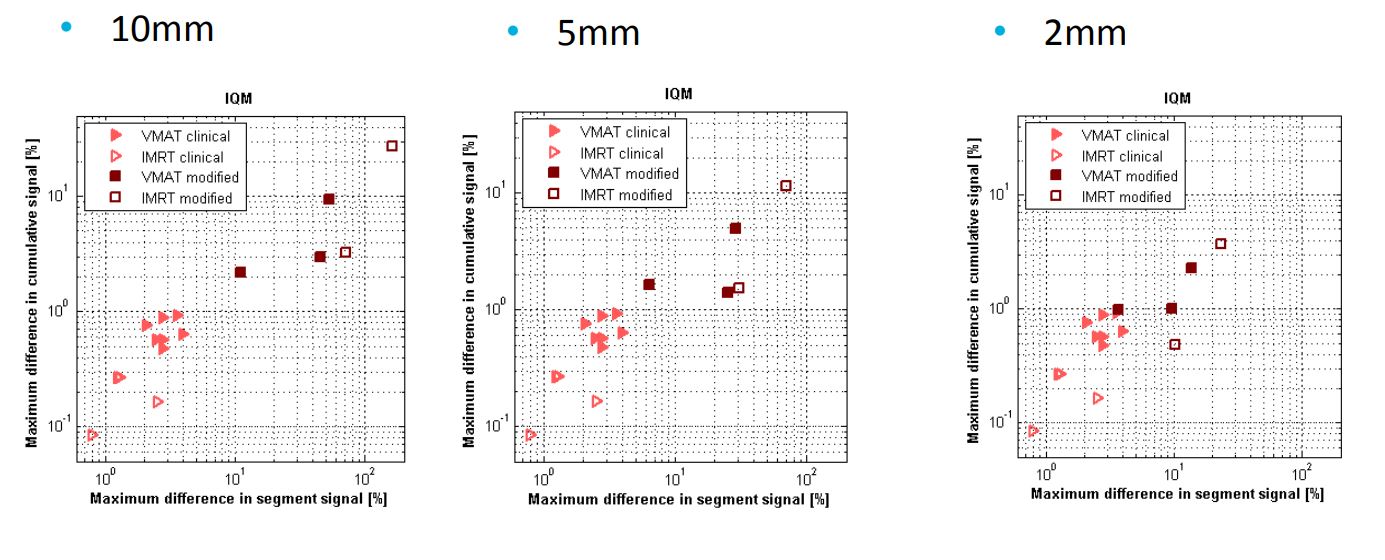
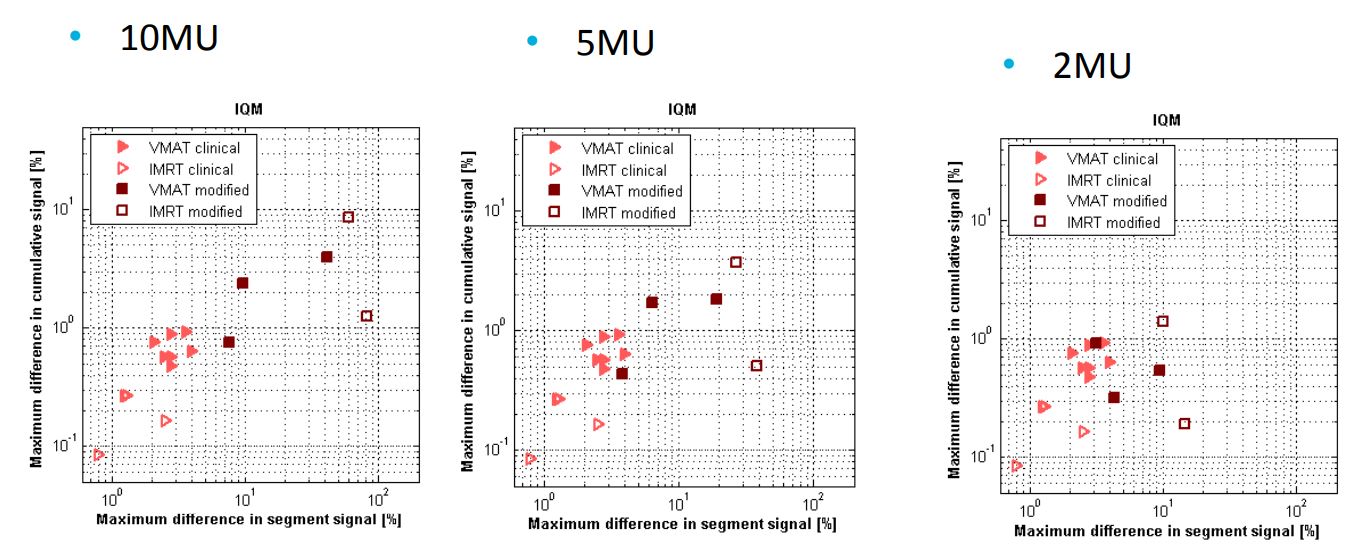
The IQM system proved to be very sensitive in detecting delivery errors. Increasing the linac output by 1MU caused a signal increase (average±1sd) of 1.0%±0.4% in the H&N cases, 1.7%±0.4% in the prostate cases and 0.5%±0.3% in the APBI cases.. The following graph shows the magnitude of signal variation detected for the seven induced errors and clearly shows that increasing dose output deviations or MLC shifts in the EI plans resulted in greater deviations between EI and EF signals.
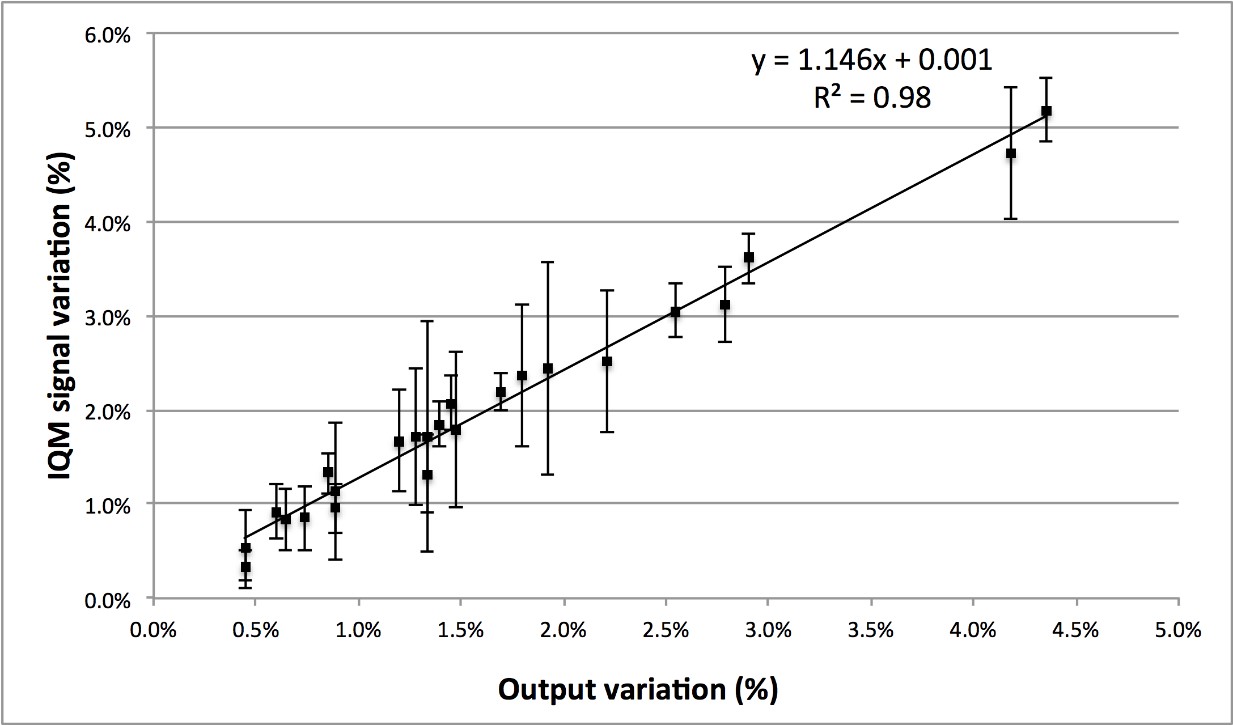
The next graph plots IQM average signal variation from reference (%) versus output variation from reference (%) for the three errors introduced on MUs for the 3 treatment sites. IQM signal correlates linearly with output.
The next graph presents an extension of the test that evaluated the IQM system’s sensitivity in detecting errors induced in the collimator jaws, orthogonal to the detector gradient. The induced MLC leaf bank position errors were repeated as collimator position errors for a prostate patient.
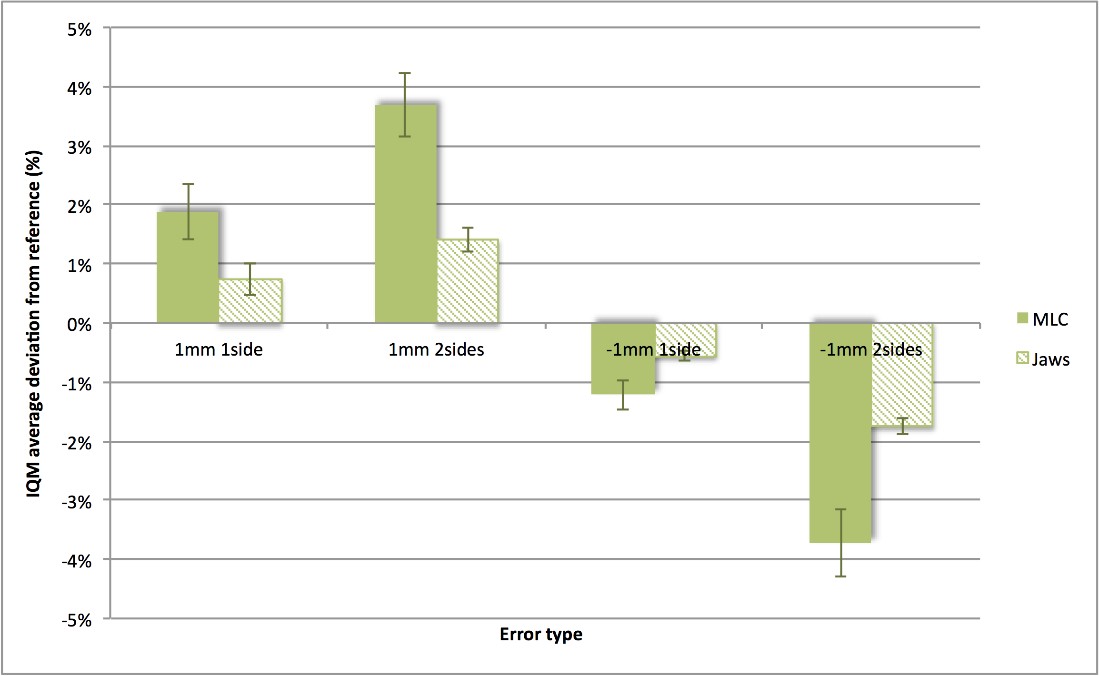
IQM is shown to be sensitive to positional variations in the orthogonal direction with respect to gradient, although the sensitivity is, on average, 1.5% less than for positional variation in the detector gradient direction.
Conclusion
The IQM detector is capable of detecting small delivery errors in MU and MLC leaf position and shows a high sensitivity for clinical practice.
Comparison of error detection sensitivity with conventional verification systems
Test purpose
This test series was intended to evaluate the error detection capability of the IQM System for a variety of clinically relevant delivery errors and compare with results of other verification systems.
Test method
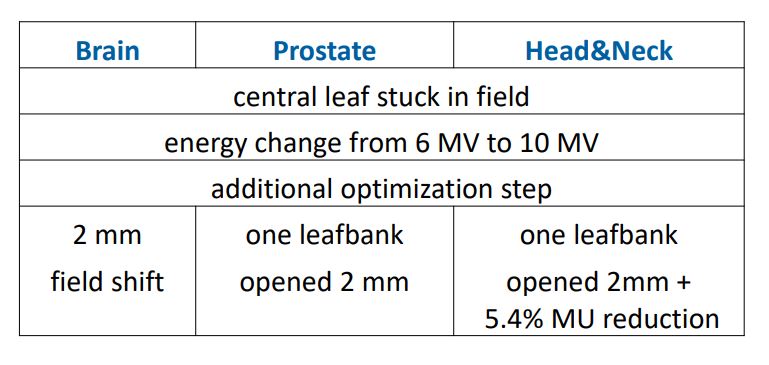
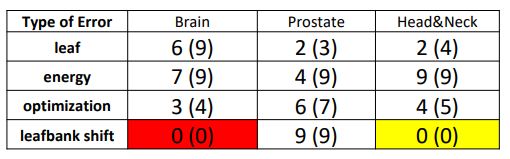
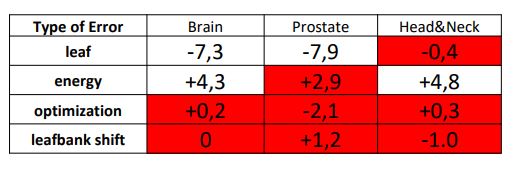
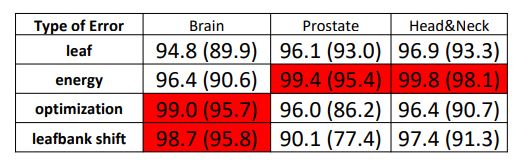
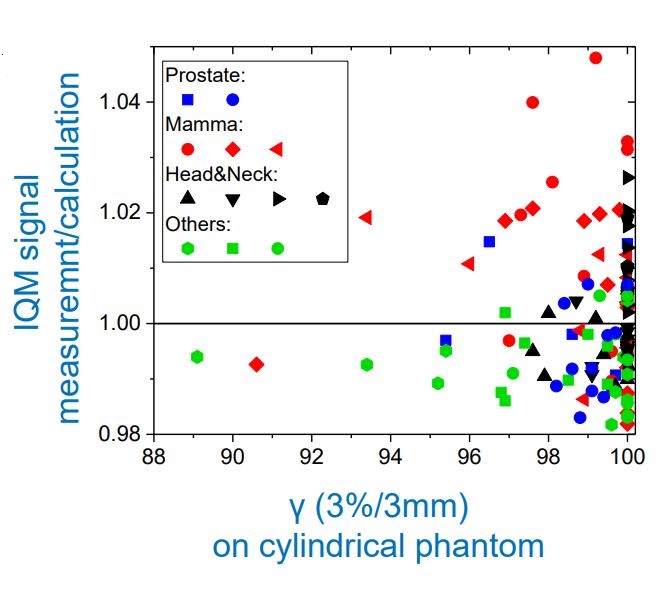
Three clinical IMRT plans were modified: Brain, Prostate, Head & Neck. All errors had a clinical effect: DVH parameters of either the targets or organs at risk changed by a few percentages. The plans were measured each with the IQM. The error detection threshold of the IQM System was set to report deviations of 3%. The modified plans were also verified with an ion chamber based cube phantom. The error threshold was defined as +/- 3%. The modified plans were also verified with a Gamma-Index based analysis using a cylindrical phantom. The acceptance criteria were set to 3%/3 mm>98% (2%/2 mm>95%).
Test results
The following tables show for how many beams within each of the 9 field plans deviations were detected by each verification method. IQM detected 11 of 12 errors, the ion chamber & cube phantom method detected 4 of 12 errors, while the cylindrical phantom with gamma index analysis method detected 8 of 12 errors. The error that was not detected by IQM was also not detected by the other two verification systems.
Conclusion
IQM showed the highest error detection rate of all three tested verification systems. During the tests only very limited user interaction was required with the IQM System. The IQM error detection was superior to the other QA procedures.

Error detection
Test purpose
Evaluate the error detection capability of the IQM System.
Test method
A variety of clinical treatment plans consisting of head & neck VMAT and IMRT cases, a larynx VMAT, a lung VMAT as well as a stereotactic lung technique were evaluated.
A number of errors were introduced at different times during the beam delivery. These errors included single segment retraction of leaves, dose changes of 10MU, 5MU and 2MU.
Test results
IQM was able to detect small errors in beam delivery with respect to a pre-calculated beam. All errors were detected without any user interaction.
Conclusion
IQM does an excellent job in real-time monitoring of beam delivery.
Sensitivity and specificity can be expected to be sufficient for clinical
practice.

Validation of calculation algorithm for clinical IMRT cases
Test purpose
Validation of calculation algorithm for wide spectrum of clinical cases, including plans with long (>26 cm) field sizes.
Test method
More than 100 fields of different plan types were measured and compared against the results calculated by the IQM calculation algorithm.
Test results
The overall agreements of the measured signal with the calculated signal was -0.2% (±1.3%). For long (> 26 cm) field sizes the agreement of the measured signal and the calculated signal is +0.4% (±1.4%).
Conclusion
IQM signal measurements agree well with the calculated references. The difference between the measured and the calculated reference signal for long field IMRT beams was slightly larger than for smaller IMRT fields. IQM can be used to verify field size of up to 40 cm x 40 cm. Very limited user interaction was necessary to achieve these results.

In-vivo dosimetry of stereotactic radiation treatment
Test purpose
To investigate the feasibility of using IQM for in vivo dosimetry of stereotactic radiation treatment with step-and-shoot intensity modulated radiation therapy (IMRT) or rotational volumetric modulated arc therapy (VMAT).
Test method
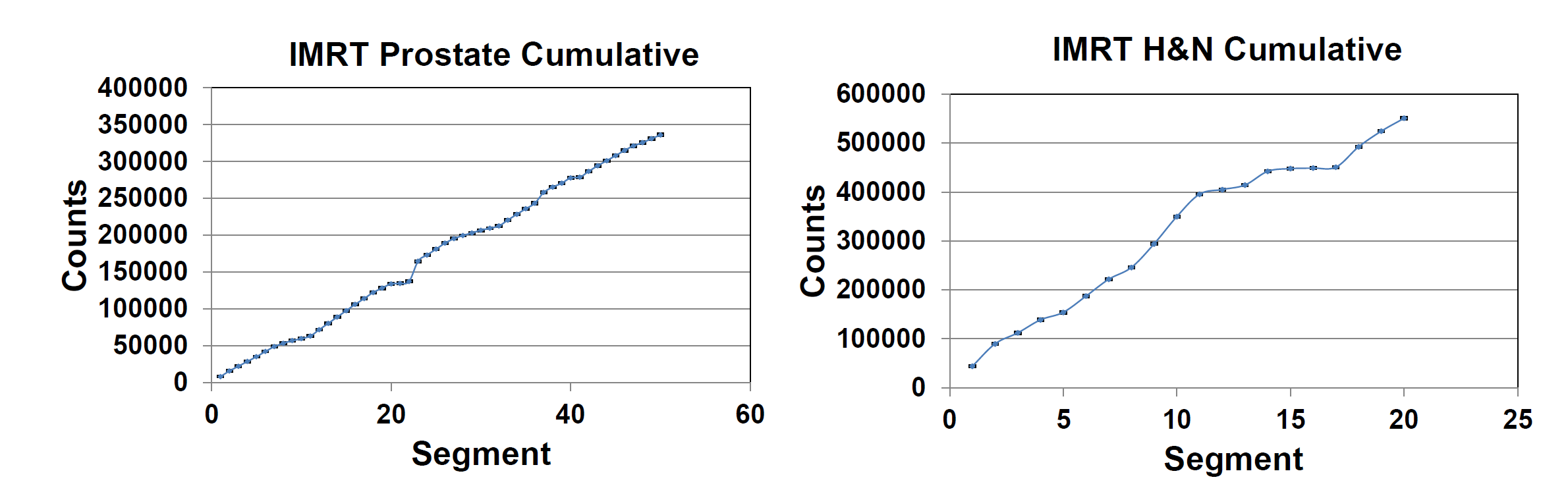
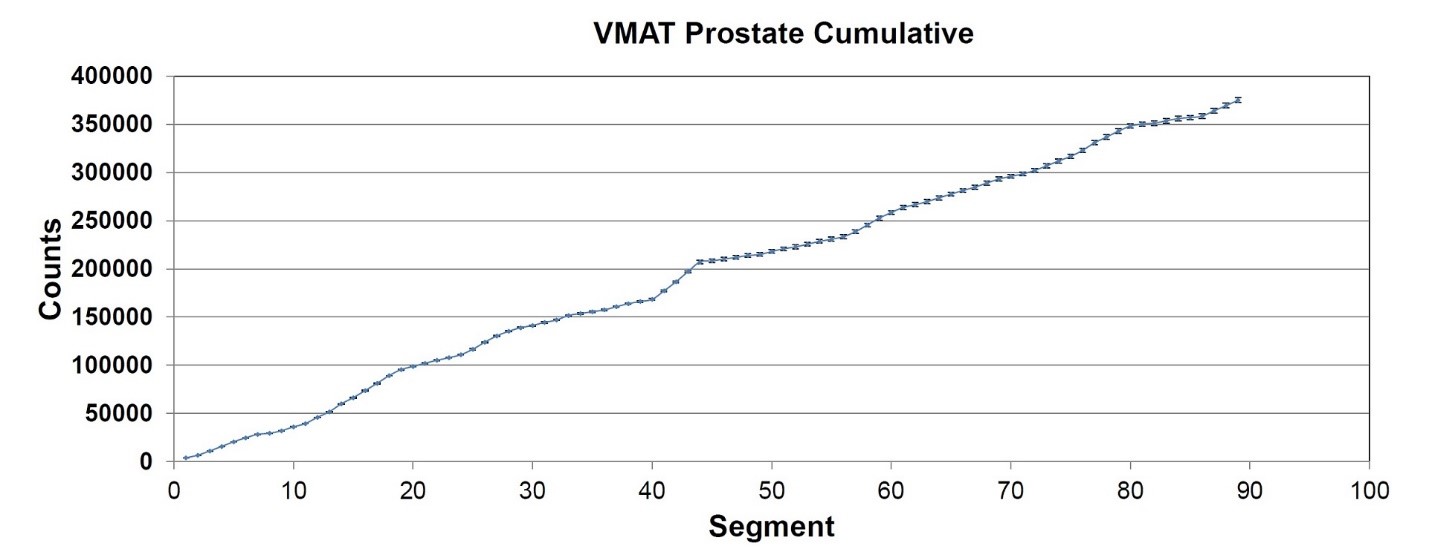
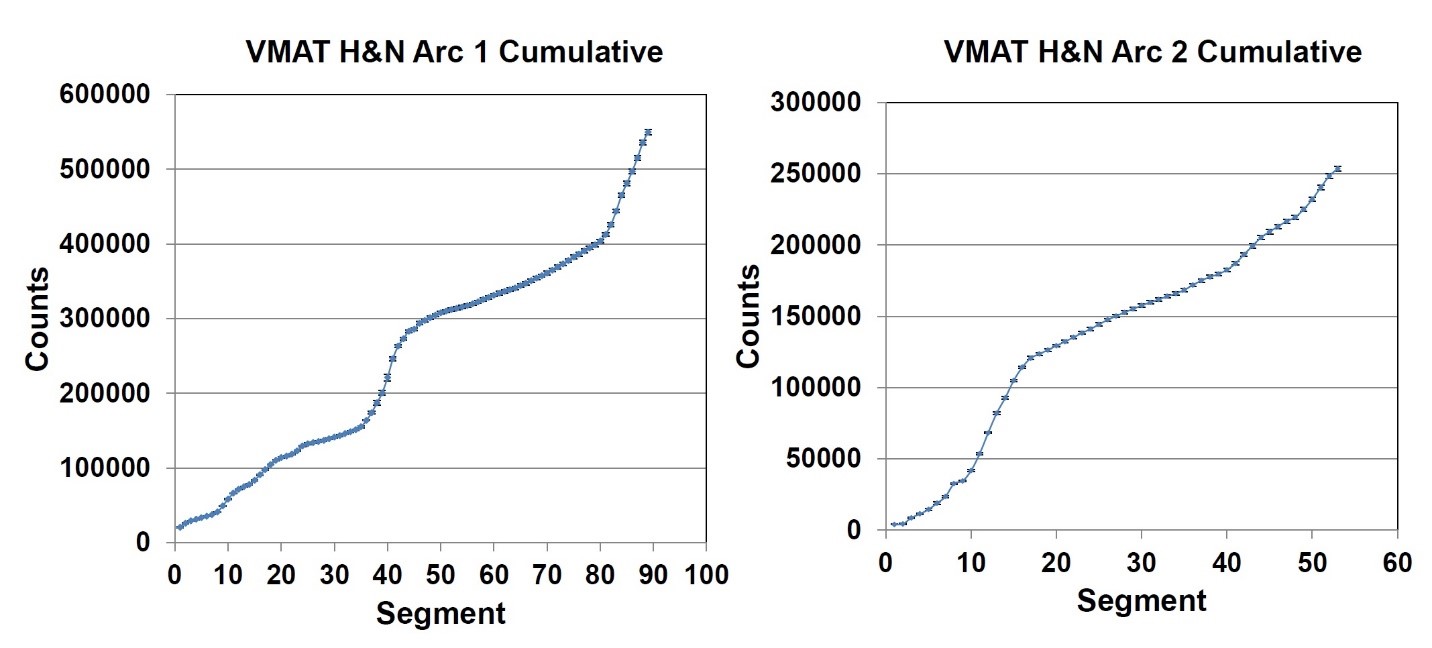
Prostate and head-and-neck IMRT and VMAT plans were used to assess IQM constancy in stationary and rotational delivering modes, respectively.
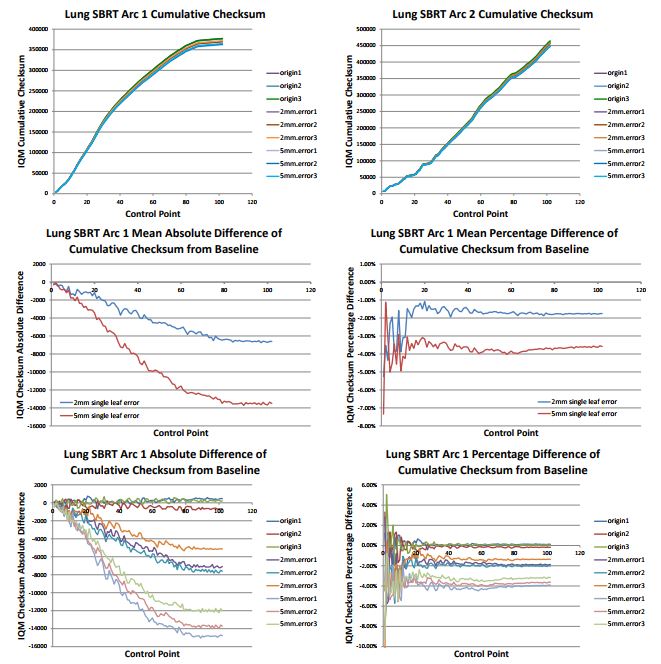
The IQM sensitivity of detecting dosimetric deviations caused by leaf errors in SBRT were evaluated with different plans. Two scenarios of plans were assessed: relatively small and large targets. Single leaf offsets of 2 mm and 5 mm into fields were introduced into the plans. Sensitivity of IQM detecting dosimetric errors in these scenarios were compared with TPS plans and MapCheck2 measurements.
Test results
IQM constancy measurements across several days showed 0.1-0.2% average standard deviation for cumulative checksum comparison in prostate and H&N IMRT deliveries and 0.7-1.0% in the tested VMAT cases.
Conclusion
IQM is a stable dosimetric system and can detect dosimetric deviations caused by small leaf errors in stereotactic radiation therapy. IQM sensitivity to leaf errors is more pronounced for relatively small fields (i.e., small targets) in SBRT and IQM appears to be more sensitive than Mapcheck2 to small leaf errors in SBRT for small targets while showing similar sensitivity in SBRT for relatively large targets.

Correlation between changes in IQM signal, Gamma-Index and DVH
Test purpose
Evaluate the correlation between changes in IQM signal, Gamma-Index and Dose Volume Histogram.
Test method
The sensitivity of detecting small delivery errors was checked by inducing seven types of errors in the IMRT clinical plans for head & neck, prostate and the IQM test plan by modifying the number of delivered MU (between 1 and 3 per beam) and by introducing deviations in linac leaf positions mimicking an MLC bank error as closing and opening one or both banks. The influence of those errors on the IQM signal, the change in Gamma Index as well as the influence on the dose volume histogram (PTV V95%) was analyzed.
Test results
IQM signal variation is plotted vs 2D Gamma per beam (1%/1mm, th10, local approach) and the PTV V95% for the H&N example. The correlation function R shows a good correlation especially with DVH parameters.
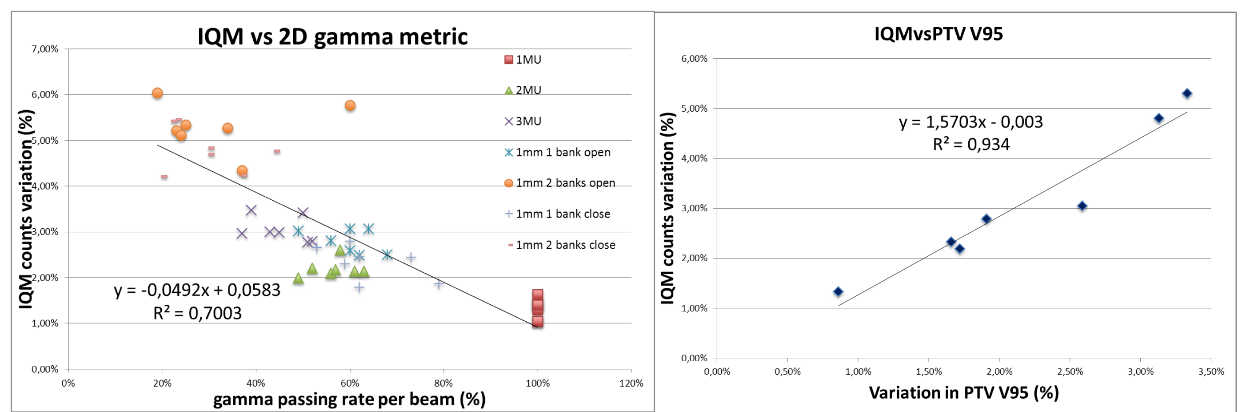
Conclusion
A good correlation between IQM signal variations and 3D Gamma, 2D Gamma and DVH parameters has been observed.

Signal constancy for IMRT and VMAT QA
Test purpose
Investigate the signal constancy of the IQM System for IMRT and VMAT plan QA.
Test method
The stationary and rotational dosimetric constancy of IQM was evaluated, using five field IMRT and single and double arc VMAT plans for prostate and head & neck (H&N) patients.
The plans were repeated three times for each measurement over several days to assess the constancy of IQM response.
Test results
Repeated IQM measurements of prostate and H&N IMRT deliveries showed 0.1 and 0.2% average standard deviation (SD) for cumulative comparison. The corresponding SDs for VMAT deliveries were 0.7, 1.3%,
Conclusion
IQM provides an effective means for real-time dosimetric verification of IMRT and VMAT treatment delivery.
Error detection sensitivity
Test purpose
Test the error detection sensitivity of the IQM System.
Test method
Errors were induced to an head & neck IMRT treatment composed by seven beams (gantry angles = 0°, 40°, 80°, 140°, 220°, 280°, 320°) generating five new treatments. Errors were induced modifying the number of delivered MU (between 1 MU and 3 MUs) and by introducing small deviations in leaf positions for each segment of each beam (mimicking an MLC bank error).
Test results
All errors introduced were detected by IQM. Errors were more easily detectable for a field of small size (approx. 6cm2).
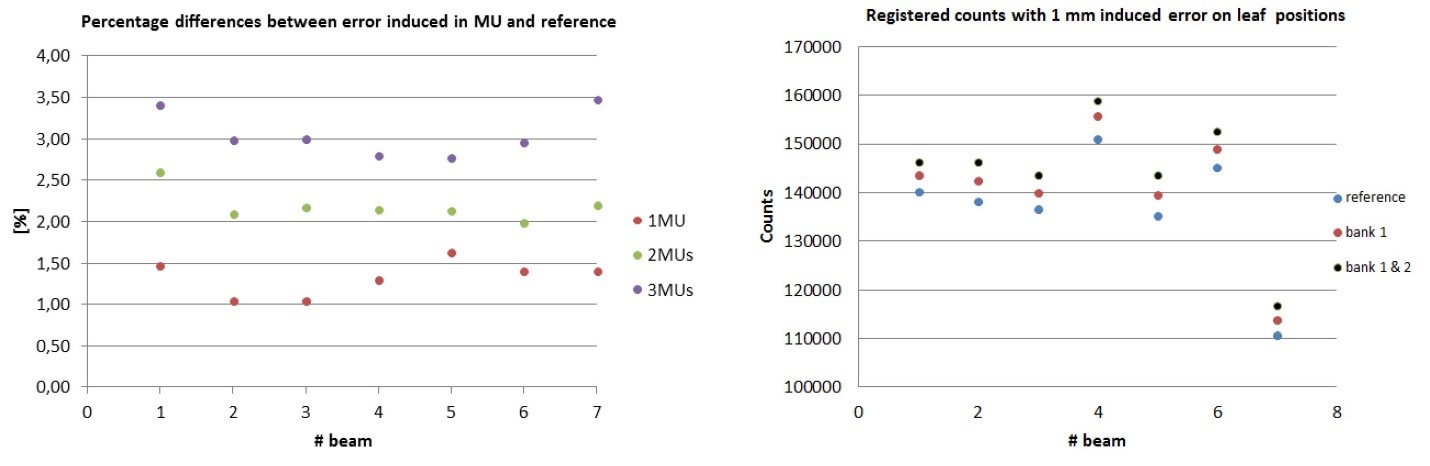
Conclusion
IQM is capable of detecting small errors in MU and leaf positions. The error sensitivity is sufficient for clinical practice.